Mandatory reporting of child abuse to protect our children
Children are not capable of protecting themselves. Early intervention in child abuse cases can effectively prevent tragedies. The Mandatory Reporting of Child Abuse Ordinance took effect on 20 January this year, requiring 25 categories of specified professionals to report promptly if they have reasonable grounds to suspect that a child under 18 has suffered serious harm or is at real risk at the course of work. Dr Lee Kwok-piu (pictured), Consultant in Paediatrics and Adolescent Medicine at Pamela Youde Nethersole Eastern Hospital, notes that there are 18 medical and health professionals including doctors, nurses, allied health professionals, and clinical psychologists, etc. The Information Technology and Health Informatics Division of Hospital Authority Head Office has created an electronic platform ‘Child Abuse Case Record’ at the Clinical Management System (CMS), which displays the reporting status of the index case to help reduce duplicated reporting efforts and facilitate internal communication. It also facilitates mandatory reporting by linking to the electronic reporting platform of Social Welfare Department (SWD) which provides decision trees for easy reference.
If a child is in immediate danger or requires urgent medical attention, colleagues should prioritise the child’s safety and clinical care, and take immediate escalation actions in accordance with hospital guidelines, e.g., call the police as appropriate, in addition to fulfilling any mandatory reporting requirement.

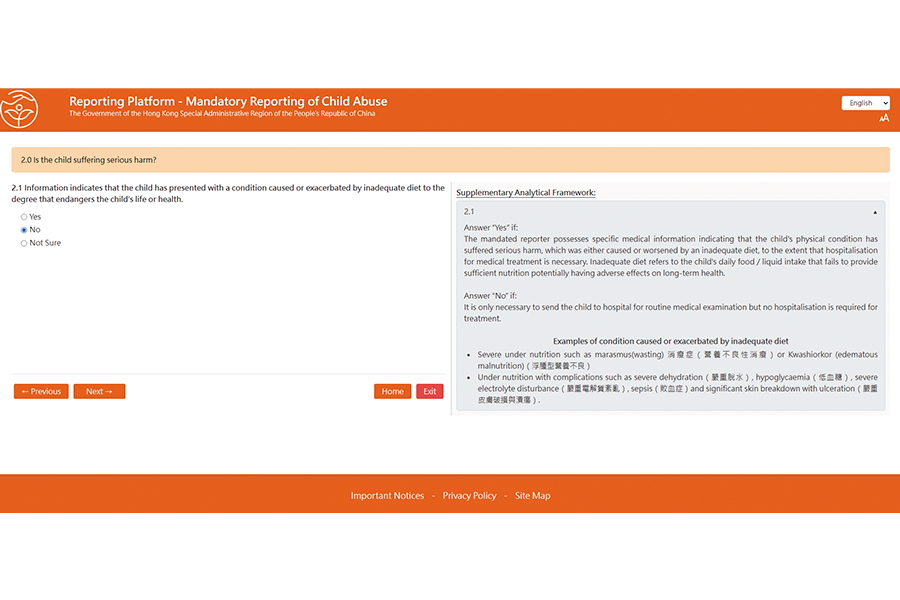 If colleagues are unsure whether the case meets the threshold for mandatory reporting, they can make reference to the decision trees and analytical framework at the SWD electronic system. Dr Lee explains: “Child abuse is broadly classified into physical abuse, psychological abuse, sexual abuse, and neglect. Each type of child abuse has its own decision tree while neglect is subdivided into four types, therefore there are totally seven decision trees supplemented by case scenarios with explanations. Colleagues should select the one reflecting the child’s most serious or primary concern.” If the result has already indicated mandatory reporting, there is no need to further explore other decision trees but to report directly to the reporting platform, where colleagues simply follow instructions to submit a written report. If uncertainty remains after reference to the decision trees, colleagues should seek advice via appropriate clinical/safeguarding escalation channels; however, where the legal threshold is met, the report should be made without undue delay.
If colleagues are unsure whether the case meets the threshold for mandatory reporting, they can make reference to the decision trees and analytical framework at the SWD electronic system. Dr Lee explains: “Child abuse is broadly classified into physical abuse, psychological abuse, sexual abuse, and neglect. Each type of child abuse has its own decision tree while neglect is subdivided into four types, therefore there are totally seven decision trees supplemented by case scenarios with explanations. Colleagues should select the one reflecting the child’s most serious or primary concern.” If the result has already indicated mandatory reporting, there is no need to further explore other decision trees but to report directly to the reporting platform, where colleagues simply follow instructions to submit a written report. If uncertainty remains after reference to the decision trees, colleagues should seek advice via appropriate clinical/safeguarding escalation channels; however, where the legal threshold is met, the report should be made without undue delay.
If a child is in immediate danger or requires urgent medical attention, colleagues should prioritise the child’s safety and clinical care, and take immediate escalation actions in accordance with hospital guidelines, e.g., call the police as appropriate, in addition to fulfilling any mandatory reporting requirement.
1. Starting from suspicious physical signs
It is uncommon for colleagues to be informed of child abuse directly by the child concerned or an accompanying person. More often, the suspicion of child abuse is triggered by abnormal physical signs. Dr Lee gives some clues for such red flag physical signs: “Infants under one year who have not yet learnt to walk should rarely have bruises from falls; new and old bruises on different body parts, and patterned injury possibly caused by canes, belts, or rulers; cigarette burns or symmetrical scalds with glove and stocking shape; bruises on abdomen or cheeks where fat is distributed. These may be red flags and should prompt further assessment and consideration of child abuse.”2. Inquiring into background from carer
Since body injuries are not necessarily caused by child abuse, Dr Lee advises colleagues to explore the reason causing the injury with the carer. “If the carer cannot provide a reasonable explanation for the injuries, or the explanations of the causes are unconvincing or contradictory to or inconsistent with the injuries sustained such as back injuries after a forward fall, colleagues should raise their awareness.” He suggests discussing with the referring clinician if no history can be taken. Where appropriate, ensure the documentation includes injury description, carer's explanation and child’s account, and follow hospital protocols on safeguarding and escalation.3. Assisting analysis with decision tree
If colleagues are unsure whether the case meets the threshold for mandatory reporting, they can make reference to the decision trees and analytical framework at the SWD electronic system. Dr Lee explains: “Child abuse is broadly classified into physical abuse, psychological abuse, sexual abuse, and neglect. Each type of child abuse has its own decision tree while neglect is subdivided into four types, therefore there are totally seven decision trees supplemented by case scenarios with explanations. Colleagues should select the one reflecting the child’s most serious or primary concern.” If the result has already indicated mandatory reporting, there is no need to further explore other decision trees but to report directly to the reporting platform, where colleagues simply follow instructions to submit a written report. If uncertainty remains after reference to the decision trees, colleagues should seek advice via appropriate clinical/safeguarding escalation channels; however, where the legal threshold is met, the report should be made without undue delay.